Introduction
Therapeutic transformation arises from the intricate interplay of psychological structure, inferential mechanisms, and lived experience. This paper proposes a tripartite model synthesizing three complementary frameworks: Personalized Self State Mapping (PSSM), which charts dissociated self-architectures (e.g. Bromberg, 1995; Steele et al., 2005; Borg, Brenner & Berry; 2022); Active Inference Therapy (AIT), which leverages Bayesian updating to minimize prediction errors (e.g. Friston, 2010; Brenner, 2025); and Experiential Field Theory (EFT), which emphasizes co-created relational fields and unconscious unity (Brenner, 2010). Grounded in complexity science and the free-energy principle, the ensuing model casts psychotherapy as emergent self-reorganization — a.k.a., self evidencing (Hohwy, 2016) — within a dyadic "analytic unity" (Brenner, 2010), where rigid priors relax via entropy-mediated plasticity (Carhart-Harris et al., 2014; Carhart-Harris & Friston, 2019), fostering integration of dissociated states (Steele et al., 2005).
While this model focuses on the psychotherapeutic interaction, it can be applied in broader understanding of clinical process to provide a framework for integrated, personalized care involving psychotherapy, conventional psychiatric medication management, and the use of brain monitoring and neuromodulation tools to support and enhance treatment; including EEG, fNIRS, TMS, tDCS and related technologies. Such technologies can provide crucial information — synchronously and asynchronously — to enhance patient outcomes and update best clinical practices.
Toward Personalized Medicine Through Continuous Assessment
Ideal healthcare would deliver economical, fast, and highly personalized treatment protocols based on detailed causal analysis of patients' biopsychosocial factors. This approach aligns with "Continuous Disease Assessment," moving beyond traditional disease classification toward what Petersen & Ursin (2025) call "fine-grained disease assessment through outcome prediction, individualized treatment modeling, and multidimensional disease characterization.” Achieving this comprises:
- Outcome prediction: Predict meaningful physiological outcomes rather than diagnostic labels
- Individualized treatment: Use causal inference to estimate individual treatment effects
- Granular characterization: Apply ML segmentation to provide detailed disease assessments and link similar cases
- Enhanced supervision: Improve model accuracy when classification remains clinically appropriate
This framework enables precision medicine that moves beyond one-size-fits-all approaches to deliver truly personalized care.
Freud’s Project for a Scientific Psychology
Drawing inspiration from Freud's (1912) metaphor of the analyst's unconscious as a "receptive organ" — attuned to the patient's transmitting unconscious — and extending his “Project for a Scientific Psychology” (Freud, 1950 [1895]; Solms, 2020), the model explores deep relational "entanglement" (Bass, 2001), extended through multi-scale temporal topologies (Buzsáki, 2025; Mousley et al., 2025). We position this as an exploratory heuristic, bridging neuropsychoanalytic traditions (Solms & Nersessian, 1999; Solms, 2018) with modern computational views, to address treatment considerations (Chamberlin, 2023; Griffiths et al., 2025), while extending to broader psychopathology.
An empirical (mechanistic) basis for mental healthcare is long-overdue, and would be expected to provide better diagnosis, improve quality of care and enhance outcomes through all phases of treatment. Current diagnostic and treatment models in mental health are generally not grounded in empirical observation and the mechanisms of empirically-grounded neuroscience. Saxe and colleagues (2022), for example, have called for a revision of psychiatric diagnosis based on a “causal diagnostic nosology”. In one study, Saxe and colleagues (2020) used Protocol for Computational Causal Discovery in Psychiatry (PCCDP) to analyze data on police trainees to identify a set of causal factors using Markovian analysis predictive of PTSD development. Their essential thesis is that causal factors should be a part of diagnosis, and that these same factors, if addressed, will necessarily lead to clinical improvement by virtue of being causal (See also The Only Cure: Freud and the Neuroscience of Mental Healing : Solms, Mark: Amazon.co.uk: Books, 2026). Interestingly, in the PTSD study, trauma was not a causal factor–while a necessary precondition, it is not part of the clinical condition itself. This is consistent with clinical data, as a relatively small fraction of people experiencing significant trauma go on to develop PTSD.
Aims include theorizing adaptive reorganization across hierarchies, leaving ample room for empirical refinement. Synergies previewed here—such as temporal coordination as a unifying thread (Buzsáki, 2025)—highlight the model's potential to reconceptualize mind as polytemporal (many times) or pantemporal (across all times), and relationally emergent. Freud's striking 1937 reference (Freud, 1937) to "psychical entropy", and related intriguing notation regarding patients with a dearth of plasticity who are not amenable to change — despite best psychotherapeutic efforts — stand out: “Our theoretical knowledge does not seem adequate to give a correct explanation of such types. Probably some temporal characteristics are concerned—some alterations of a rhythm of development in psychical life which we have not yet appreciated." [italics added] Emerging technologies including digital twinning and causal diagnostic modeling of brain activity are promising avenues to realize such formerly purely speculative approaches (e.g. Kita et al., 2025).
Psychodynamic and psychoanalytic therapies are characterized by the following seven areas of focus (Shelder, 2010) including: Focus on affect and expression of emotion; Exploration of attempts to avoid distressing thoughts and feelings; Identification of recurring themes and patterns; Discussion of past experience (developmental focus); Focus on interpersonal relations; Focus on the therapy relationship; Exploration of fantasy life. Short-term structured therapies such as cognitive behavioral therapy and a range of other second, third and fourth wave therapies are often presented as “evidence-based”, though as with psychiatric medications, the length of study follow-up is often short. Less well known is that traditional long-term talk therapy (first wave) has a body of data supporting its efficacy, both it the short-term, and to the point of our discussion, persistent and deepening after therapy has stopped, with studies ranging over several years (e.g. Shedler, 2010; Leichsenring et al., 2023). The elegance of Freud’s (2012) basic therapy “algorithm” is informative: The patient moves toward “free association”, attempting to learn to speak uncensored in the presence of the therapist.
The therapist, complimentarily, practices “evenly suspended attention”, not filtering data from the patient in any way, to the best of their ability. Particularly with awareness of their own responses’ liability for introducing distortion, and with appropriate training and supervision:
"[M]ust adjust himself to the patient as a telephone receiver is adjusted to the transmitting microphone. Just as the receiver converts back into sound waves the electric oscillations in the telephone line which were set up by sound waves, so the doctor's unconscious is able, from the derivatives of the unconscious which are communicated to him, to reconstruct that unconscious, which has determined the patient's free associations."
The final aspect is the “frame” of therapy–the basic set of expectations of both a pragmatic nature such as fees and scheduling, as well as the expectation to work as above, with the goal of assisting the patient.
Clinical Context: TMS-Assisted Psychotherapy (TAP)
For clinical context — illustrating neuromodulation with long-term therapy — here is a composite of people treated with off-label accelerated TMS protocols presenting with a familiar combination of: treatment resistant depression, complex PTSD and dissociative symptoms, not meeting full DID criteria but experiencing "parts" of themselves to varying degrees of concreteness, interfering with life satisfaction and therapeutic progress (difficulty making more than intellectual changes, frustrating helpless feelings, being aware but unable to change leading to worsening of depression). Characteristically, people spend years struggling with "self-hating parts" shaped by complex trauma—an intrusive critic with an antagonistic aspect, interfering with day-to-day function and self-esteem, often reminiscent of early critical developmental figures, characterized by patterns of self-approach and self-avoidance.
When we integrated a TAP-style sequence (Brenner, Ufearo & Zhou, 2025)—personalized rTMS synchronized with psychotherapy within the post-stimulation plasticity window—the shift was typically dramatic. Within the first week, intrusive thoughts quieted abruptly; patients report feeling "surreal" and "weird," unable to believe the difference. As neuroplasticity accelerated, what had seemed like a fixed "part" dissolved into process: insights arrived faster, dissociative distance softened, and self-criticism resolved into reflective function. They emerged convinced by how "real the brain is"—an awakening often described as an experience of personal revelation, useful therapeutically — if existentially de-centering — by demonstrating the brain-as-organ, and therefore treatable, versus more ineffable models of mind. TAP offers a tractable path to test these shifts: using neuromodulation to open a window, then psychotherapy to consolidate change, from fragmented parts into coherent self.
TAP Core Elements:
- Combines rTMS with psychotherapy during post-stimulation neuroplasticity windows. Psychotherapy may also help patients work toward seeking treatment with modalities such as TMS, as patients often are hesitant about psychiatric care, making psychotherapist education about neuromodulation an important priority.
- Personalizes targeting and protocols to patient's symptoms and functional anatomy.
- Aligns psychotherapy modality to stimulated circuits (e.g., cognitive work with DLPFC, affect regulation with limbic).
- Phases: preparation/personalization → synchronized stimulation + therapy → consolidation/maintenance → optional retreatment.
- Aims beyond symptom relief toward "bending the developmental curve"—fostering lasting internalization and growth by leveraging psychotherapy in the mid to long-range post-treatment phase.
- Adding to the current paradigm of acute treatment, rescue/booster and maintenance treatment, developing the concept of a “tail” to extend the neuroplastic window. For example, providing acute accelerated TMS and additional less frequent stimulation sessions afterward, and/or using modalities such as tDCS, tACS and/or medications which impact plasticity to extend the window of opportunity. Understanding the mechanisms of various treatments and the duration of neuroplasticity is essential for this type of application.
- TAP may be generalized in future iterations, broadly as “Neuromodulation-Assisted Psychotherapy” (NAP).
Core Elements of the Tripartite Model
Experiential Field Theory (EFT): The Phenomenological Ground
EFT posits psychological reality as fundamentally experiential—"how you look at it and what you make of it" (Brenner, 2010): The approach here is deeply informed by my training at the William Alanson White Institute of Psychiatry, Psychology & Psychoanalysis in New York City, in addition to classical psychoanalysis, in the Interpersonal-Relational tradition.
Without going into detail, founders of the Interpersonal tradition, such as psychiatrist Harry Stack Sullivan (who developed an alternative to Freud), grounded their theory in dynamics between and among individuals rather than the classical psychoanalytic focus on individual, or “intrapsychic” processes. Interpersonalists drew from social theories, systems theories, and foundationally for Sullivan, the physicist Percy Bridgman’s theory of Operationalism: “[W]e mean by any concept nothing more than a set of operations; the concept is synonymous with the corresponding set of operations” (Bridgman, 1927).
Likewise rooted in autopoietic theory (Maturana and Varela, and nonlinear dynamics as a metaframework (Seligman, 2005), EFT emphasizes operational closure: each individual's field is complete, with therapeutic work occurring through synchronisation with the analyst's experience to form an analytic unity with emergent properties (e.g., shared rhythms; Brenner, 2010). Key elements include strange attractors (recurrence and reciprocal causation in patterns; Brenner, 2010) and nonlinear dynamics (bifurcations, phase transitions and self-organised criticality). Language serves as a medium—like "paint to art"—requiring nonverbal channels for full synchronisation [of chaos] (Tschacher et al., 2017; Tschacher and Haken, 2007).
EFT fosters the unity's evolution, where dissociated material emerges as field perturbations (Holmes & Nolte, 2019), aligning with relational psychoanalysis's "analytic third" (Ogden, 1994). Inspired by Freud (1912), the analyst's unconscious acts as a "receptive organ" for the patient's transmitting unconscious, echoing Bass (2001)'s "dialogue of unconsciouses." This phenomenological ground supports imagination over dissociation, and views narrative truth as co-constructed, in the tradition of Gadamer’s hermeneutics (Gadamer, 1975). See (Friston and Frith, 2015) for a simulation of co-constructed narratives — via generalised synchrony — under active inference.
Clinically, this model is generally applicable, though the focus is on a broad psychoanalytic framework, within which more structured models can be located and elaborated. Arguably, the basic algorithm of psychoanalysis articulated by Freud (1912) of cultivating free association for the analysand, and evenly suspended non-selective attention by the analyst, generates a therapeutic, higher-entropy, psychedelic-like space for conjoint exploration.
Active Inference Therapy (AIT): The Mechanistic Engine
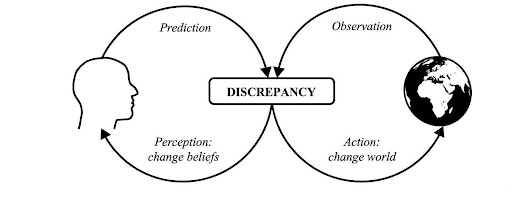
AIT frames therapy within the free-energy principle: organisms minimize surprise by updating priors or acting to align expectations with reality (Friston, 2010; Friston et al., 2014; Brenner, 2025). Humans as "telonomic matter", a term coined to suggest purposeful matter, also “agential matter” (Levin, 2019), pursue self-evidencing through active inference, with psychopathology as rigid, overly precise, priors resisting update (Chamberlin, 2023).
Psychoanalytic psychotherapy has been discussed extensively (Holmes, 2024; Solms, 2024) in the context of Karl Friston’s work on free energy, highlighting the role of active inference as ways, respectively, of making and testing predictions based on perceptions of the “likely state of the world, and testing and updating those predictions via action and/or agency. This minimizes free energy, precluding surprising exchanges with the world, and building negentropy locally, while respecting the Second Law of Thermodynamics.
Holmes goes into detail regarding specific psychoanalytic processes related to transference, a key concept in psychoanalysis in which patients import distortions from developmental experience into the therapeutic relationship and perceive the therapist as possessing characteristics of early caregivers, typically in ways which allow dysfunctional beliefs and memories to be rectified. Holmes references canonical work of Donald Winnicott (1953) regarding “transitional space” and the poet John Keat’s concept of “negative capability”, regarding William Shakespeare: ‘when a man is capable of being in uncertainties, mysteries, doubts, without any irritable reaching after fact and reason’. This concept is widely used in contemporary psychoanalysis in certain circles, referring to relational models and “duets for one” in generalised synchrony (i.e., free energy minimising synchronisation of chaos), discussed briefly below. Finally, he notes the importance of unbounded free energy in the present moment, as “necessary uncertainty” driving an active reduction of surprise, leading to exploration or “epistemic foraging” of the lived world to update our world models.
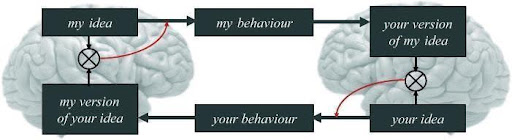
Friston and Frith (Friston & Frith, 2015), discuss the duet for one framework for synchrony in shared inferential processes, providing a way to understand theory of mind as a mathematical basis for “communication as generalised synchrony” of neuronal processes involved with “attention to and attenuation of sensations”, as shown in Figure 1.
Core elements include predictive processing, dyadic inference (coupled therapist-patient updating), and circular causality (recursive loops shaping experience), mediated by causal Markov blanket boundaries (Friston, 2010), within which the analytic process influences outcomes through direct experiential access, shifting perception, action and world models of reality and person in the world. When individual experience shifts and updates, new worlds become possible which beforehand were inaccessible and — under old priors — were perceived as impossible. Here, the therapeutic relationship (“analytic unity”; Brenner, 2010) is conceptualized as a coupled dynamical system with causal impact, where patient and therapist engage in mutual active inference (interactive inference) to minimize surprise and foster adaptive self-evidencing.
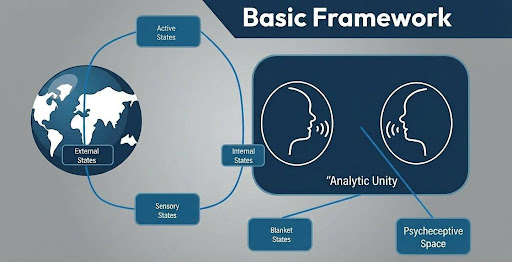
This "analytic unity" operates within a bounded space—the therapeutic frame—functioning as a Markov blanket that contains all necessary information for causal inference within the system, providing mathematical precision to psychoanalytic notions of shared relational fields (Figure 1). Following the work of Parr, Pezzulo and Friston (2020), AIT introduces "psycheceptive space" as a liminal domain in which conjoint exploration occurs (Figure 2).
Figure 1
Between interoceptive and exteroceptive experience, nested within the Markov blanket where causal influences are strongest, the psycheceptive space serves as a key environment for developmental changes through actions that reshape internal models. In psychoanalytic terms, the relates to Winnicott’s aforementioned notion of the “transitional space, as well as Bion’s notion of a “container” (Bion, 1962). This space is neither purely internal nor external but represents the co-constructed reality of the encounter, enabling both participants to engage in "co-self-evidencing" by utilizing data from within and beyond the therapeutic frame to update predictive models and promote integration.
Figure 2: World-Analytic Unity Interactive Inferential Relationship
AIT unfolds in five recursive phases: Capture (baseline coupling), Initial Evidencing (calibrated errors), Working (model consolidation), Release (internalization), and Post-Termination (monitoring). It incorporates multi-clock hierarchies—from fast sensory updates to ultraslow self-models (Brenner, 2025; Buzsáki, 2025, and earlier) —paralleling PSSM's self-continuity scales for temporal coordination, while EFT's fields provide the relational container for mutual updating. Freud's (1937) "depletion of plasticity" as psychical entropy links to AIT's minimization, enabling adaptive posteriors (Holmes & Nolte, 2019).
Personalized Self State Mapping (PSSM): The Structural Architecture
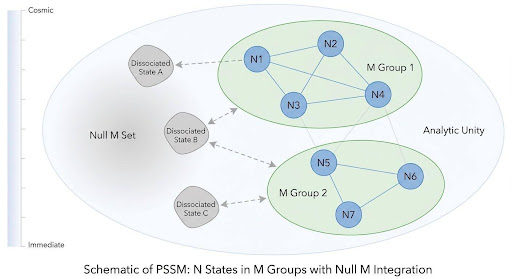
PSSM conceptualizes personality as N parts organizing into M clusters (Figure 3), evolving developmentally across nine scales of self-continuity (Table 1), drawing on the work of Philip Bromberg on multiplicity of self-states in interpersonal-relationship psychoanalysis (Bromberg, 1998) and the structural theory of dissociation of the personality (van der Hart, Nijenhuis & Steele, 2005; van der Hart, Nijenhuis & Steele, 2006) and the treatment of persons with complex trauma and dissociative disorders (Kluft and Fine, 1993).
Table 1: The PSSM model identifies nine interconnected scales of self-continuity, and a tenth “wildcard” of imaginary selves, which in some ways may be the most important as it is a fulcrum for change.
| Scale | Temporal/Contextual Scope | Key Focus |
|---|---|---|
| Immediate Self | Momentary awareness | Present-moment sensory/emotional experience |
| Short-Term Self | Hours/daily experiences | Daily routines, transient emotions, and adaptive responses |
| Contextual Selves | Social identities across settings | Role adaptability, Interpersonal Selves (e.g., parent, professional, friend) |
| Extended Self | Days/weeks + personal narratives | Coherence of life stories and identity integration |
| Long-Term Self | Months/years + life stages | Developmental transitions (careers, relationships) |
| Lifetime Self | Full arc of existence | Legacy, existential meaning, and life review |
| Ancestral Self | Generational continuity | Intergenerational trauma/resilience and family narratives |
| Collective Self | Species-wide identity | Shared human experiences and cultural belonging |
| Planetary/Cosmic Self | Earth/universe connection | Ecological/spiritual interconnectedness |
| Imaginary Selves | Various | False, Aspirational, Suggested or Imposed Identities, Dissociated, Fantasied, Psychotic, Possible, etc. |
Key elements include parts/clusters (with boundaries as flux zones), Null M sets (dissociated potentials), and a six-stage process: Education, Context-Building, Goal Clarification, Mapping, Transitional Scaffolding, Iterative Installation. PSSM operationalizes phase-oriented treatment (Griffiths et al., 2025; Steele & Hart, 2010), overcoming phobias through reorganization, with scales addressing temporal mismatches (Buzsáki, 2025; Mousley et al., 2025 for lifespan topology).
Figure 3: N Self-States in M Clusters, with Null M Set of Dissociated Parts
PSSM is intended to be useful on a continuum from concrete to metaphorical; specifically, to allow for containing people with strong dissociation resulting in multiple dissociative parts of the self. These parts may be experienced subjectively as distinct, autonomous entities despite being part of one person in one body, and for more literary or conceptual use — for people with a more coherent sense of self – to consider ways to build better “self-relationship (Borg, Brenner & Berry, 2022). For example, with explicit recognition of the serious risk of inducing fragmentation by overzealous application of concrete therapeutic models while maintaining the potential benefits of making the “whole greater than the sum of the parts” through integrative work.
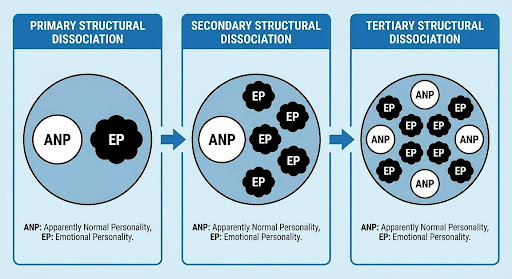
Drawing from structural dissociation, dissociation may be viewed as failed integration of action systems (defense vs. daily life) which fracture along psychobiological lines (e.g. fight-flight, freeze, fawn), mapping "apparently normal parts" (ANP) and "emotional parts" (EP), shown in Figure 4. In primary structural dissociation, there is one ANP and one EP, in secondary one ANP and two or more EPs, and in tertiary two or more ANPs and EPs. Therapeutic work increases functional coherence — i.e., synchronisation — through building internal connections leading to both integration of parts, and communication among parts e.g. merger and/or co-consciousness. Formal network mapping tools e.g. the Jaccard Similarity, may be useful for formalizing the relationship between internal self-state architecture and neural networks.
Figure 4: The Structural Theory of Dissociation
PSSM extends the work started in the self-other-help book Making Your Crazy Work For You: From Trauma and Isolation to Self-Acceptance and Love (Borg, Brenner & Berry, 2022) and notably is an alternative to the popular Internal Family Systems model (IFS; Schwartz, 1995), specifically in offering a more open, adaptive, individually-originated and personalized model than the pre-formed structure in IFS of firefighter, manager and exiled children, under the aspirational idea of Self, which we consider having risks associated with suggestion and forced-fit, a full discussion of which is beyond the scope of the current discussion.
An important element of the model is the recognition not only of different self-states within a structural framework, but how these states evolve over time, and notably how different self-states may experience time differently. We have made the point elsewhere (Brenner, 2025) that part of developing personality integration recognizes that sense of time may vary from self-state to self-state, and that there needs to be a level of coordination among different self-states which takes into account synchronization, and approaches to connecting self-states which may be disconnected in subjective temporal experience. For example, some self-states may experience timelessness (contemplative states) or frozen time (paralyzed or traumatized dissociative states), while others may live in lineal clock and calendar time, while others experience time in fractal, nonlinear ways. This is addressed further in Experiential Field Theory as subjective experience within a complex, adaptive framework can hold multiple centers of experience and sense of time.
Theoretical Overlaps, Differentiations, and Synergies
All frameworks converge on self-organization within a moderated developmental context, or psychotherapeutic frame: systems evolve adaptively under constraints, constraints which may both enhance developmental potential or limit it. EFT's field exclusions align with AIT's fragmented models and PSSM's Null M sets (Chamberlin, 2023). Nonlinear dynamics unite them: EFT's attractors are AIT's free energy minima and PSSM's boundary flux (Brenner, 2010). Relational context is essential—EFT's unity, AIT's dyadic synchronisation, and PSSM's inter-part dialogue emphasize co-creation (Holmes & Nolte, 2019; Bass, 2001), with Freud's aforementioned (1912) "receptive organ" metaphor underscoring unconscious linkages.
Temporal hierarchies converge and are critical to therapeutic process, as time and change bind mind and behavior: PSSM's scales align with AIT's multi-clock processing (Brenner, 2025) and EFT's self-similar patterns, enabling coordination of immediate (reactive) and extended (reflective) self-states (Buzsáki, 2025; Mousley et al., 2025 for topological turning points across lifespan). Freud's (1937) "psychical entropy" and depletion of plasticity highlight developmental limits, tying to AIT's free energy minimization and Solms and Panksepp's (Solms & Panksepp, 2012) affective neuroscience.
Differentiations include levels of analysis: EFT phenomenological (lived field), AIT mechanistic (predictive computation), PSSM structural (parts architecture). Change metaphors vary: EFT emergent fields, AIT error minimization, PSSM boundary reorganization.
Synergies emerge at multiple levels: structurally, PSSM's parts/clusters as AIT's generative models, manifesting in EFT's fields; mechanistically, AIT's updating via self evidencing resolves PSSM's Null M, facilitated by EFT's dialogue; phenomenologically, EFT's unity enables AIT's inference and PSSM's scaffolding. Temporal themes unify: poly-temporal topology bridges models, with Freud's rhythms of development and Mousley and colleagues’ brain development network analysis suggesting predictable adaptive reorganization across scales. The goal of psychotherapy and related interventions (e.g. neuromodulation-based approaches including transcranial magnetic stimulation, see also Brenner and colleagues’ model of TMS-Assisted Psychotherapy in Neuromodec Journal
Integrated View and Meta-Framework
The tripartite model forms a meta-framework for psychotherapy as multi-level self-reorganization, synthesizing structural (PSSM), mechanistic (AIT), and phenomenological (EFT) views. At its core, mind emerges from poly-temporal topology, where hierarchical brain-body rhythms coordinate unformulated experience (Stern, 2009) into adaptive configurations. Freud's "psychical entropy" aligns with AIT's minimization of surprise/free energy, while PSSM's scales map developmental turning points catalyzed by greater efficiency in internal information process and connectivity, grounded in EFT's relational crucible, which provides the an experiential, conjoint psycheceptive space for exploration and testing of fantasy and reality: translating to external change via play, experimentation and model testing and updating, in a recursive process leading to consolidation, internalization of the psychotherapeutic process, and termination. This integrated model aspires to fully update the patient’s “operating system” to be both more adaptive to the current environment, as well as capable of adapting to changes across the lifespan and identify when to resume therapy.
Vertical integration: PSSM provides architecture (parts as priors), AIT mechanisms (belief updating), EFT experiential ground (fields for emergence). Dynamical emergence enables synergies, such as AIT's clocks resolving PSSM's Null M through EFT's partly intentional, partly implicit, blending of conscious and unconscious processes in the shared, co-emergent experiential field. This framework positions therapy as fostering curiosity and play, while also maintaining a rational framework to provide containment and directionality for a complex, often unruly process.
Integrating Neuromodulation and Psychotherapy: A Speculative Moment
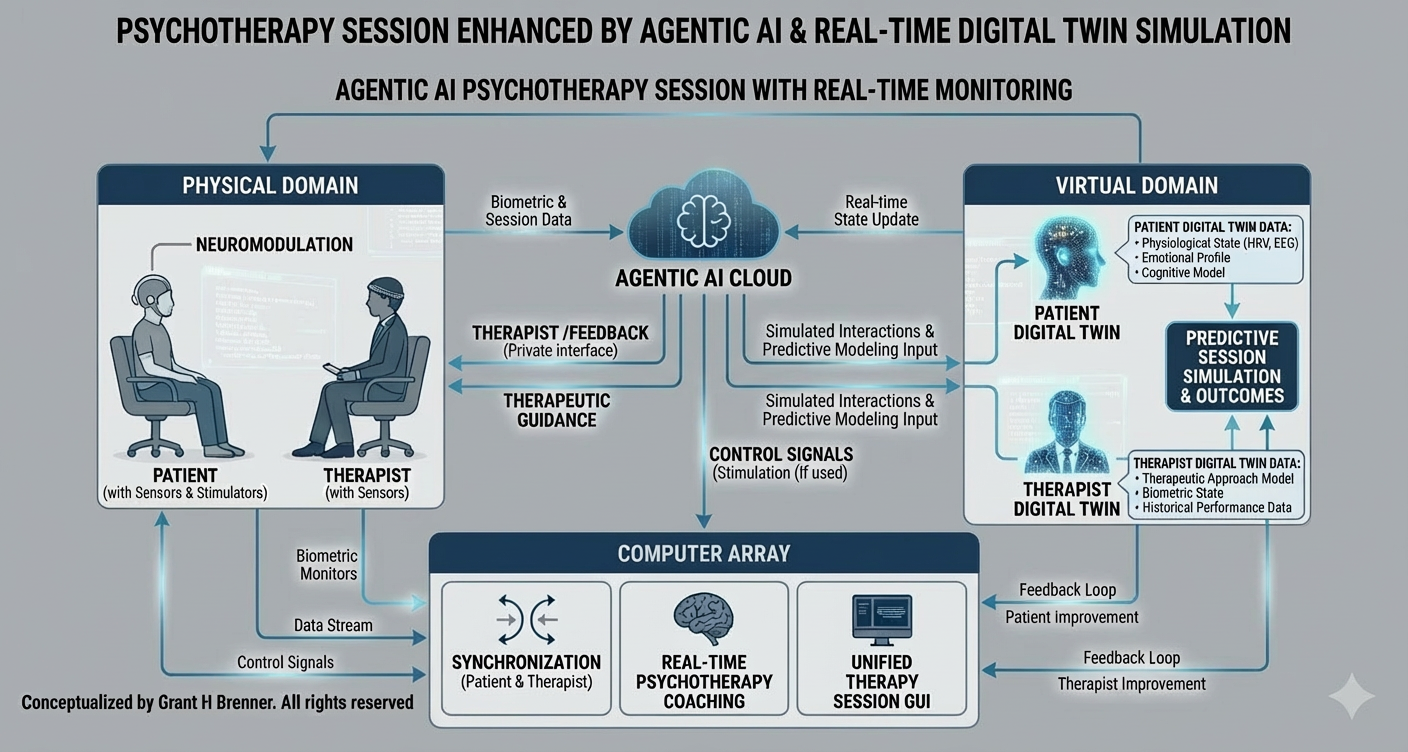
Emerging neurotechnologies are likely to become a crucial element in causal diagnostic discovery and related treatment, both in terms of interventional psychiatry and neuromodulation more generally, as well as for informing treatment planning and providing crucial information for use in psychotherapeutic processes. For example, in a near-future science fiction-type scenario, therapist and patient could incorporate data from outside of sessions to inform clinical focus on causal factors within sessions (Fig. 5). Likewise, real-time monitoring during therapy could be used to guide focus of therapy, helping the pair to remain engaged in ways which have highest impact, and identify when the process is straying into ineffective or defensive areas.
Michael Levin's research (Levin, 2021) demonstrates that bioelectrical fields direct embryological processes, store organism-level memory (e.g., flatworm head number), and can revert cancer cells to normal behavior without altering genetic mutations. This works by restoring cellular communication, allowing rogue cells to rejoin the collective "cognitive glue" rather than exploiting the body as free agents.
Looking forward, Levin envisions an "anatomical compiler" (Lagasse & Levin, 2023) that could reshape organic matter, including human bodies, according to desired specifications. As Levin explains: "Some day, you will be able to sit down in front of a computer and draw the animal, plant, organ, biobot, etc., that you want... The anatomical compiler will convert that anatomical description into stimuli that have to be provided to cells to get them to build exactly that" (Brenner, 2025).
Predicting and Managing Therapeutic Alliance
Early research on using fMRI scans while participants watch emotionally valanced videos presents intriguing possibilities for psychotherapy. Researchers found that whether participants will be friends eight months later can be predicted, and is correlated with and likely causally-related to participants’ neural similarity in key brain areas, notably the left orbitofrontal cortex (Shen et al., 2025). Those who grew closer over time showed increasing similarity in canonical networks, including default mode, frontoparietal control network and the dorsal attention network. While the patient-therapist relationship is not a friendship, this work suggests the intriguing possibility of predicting therapeutic relationship fit to select for more likely positive outcomes, tracking development of the therapeutic relationship, and even intervening when it starts to diverge, or enhancing the effectiveness of care via a range of interventions.
Figure 5: AI and Neuromodulation Assisted Psychotherapy: A Speculative Framework
Future Directions
Psychodynamic Therapy and Neuromodulation
The convergence of the tripartite model with emerging neuromodulation approaches, particularly as discussed in TMS-Assisted Psychotherapy / Neuromodulation-Assisted Psychotherapy (TAP/NAP; Brenner et al., 2025), suggests numerous testable hypotheses. Building on observed qualitative differences in ego function enhancement following TMS—distinct from other neuroplastic interventions—we propose that targeted neuromodulation can facilitate the integration of PSSM structures, AIT mechanisms, and EFT fields through measurable neurobiological pathways. Apart from the tripartite model presented here, which is not in common use or for that matter an established paradigm, accepted psychodynamic and psychoanalytic approaches as currently in use can be researched in combination with present-day and emerging neuromodulation approaches to treatment and monitoring, developing neurobiomarkers for predicting personalized outcomes, and tracking for response to intervention for ongoing optimization of treatment plans delivered over longer time-spans.
Core Hypotheses:
- Enhanced Reflective Function: TMS-induced neuroplasticity produces measurable improvements in mentalization, theory of mind, and therapeutic engagement that exceed those observed with pharmacological interventions alone.
- Differential Neuroplastic Signatures: Neuromodulation creates qualitatively distinct patterns of neural reorganization compared to ketamine or conventional antidepressants, specifically enhancing top-down cortical control and reducing subcortical rigidity.
- Therapeutic Priming Effects: Psychodynamic interventions can optimize pre-TMS states to enhance neuroplastic responsivity, while post-TMS windows enable deeper psychodynamic processing.
Connectivity Mapping
Drawing on established neurobiological research in dissociation, particularly findings of altered functional connectivity patterns in the prefrontal cortex, amygdala complexes, insula, and hippocampal regions across dissociative disorders (Lanius et al., 2018), PSSM configurations may exhibit measurable neurobiological signatures. Recent neuroimaging studies have identified affected brain regions in frontal grey and white matter, with clinical relevance for DID diagnosis (Reinders et al., 2018), suggesting that self-state architectures may be detectable through accessible neuroimaging. Recently, researchers (He et al., 2025) mapped brain networks activated by TMS using fMRI and EEG (fET, together), showing stronger activation in key networks by timing to frontal cortex alpha rhythms, and baseline evoked responses predicted clinical response in the synchronized group. Notably, there were no significant differences between synchronized and non-synchronized group antidepressant clinical outcomes.
Core Hypotheses:
- Connectivity-State Mapping: Parts-based architecture correlates with specific dysconnectivity patterns, particularly in fronto-limbic networks where subcortical white matter alterations have been identified in dissociative conditions (Ross et al., 2021).
- Accessibility Through fNIRS/EEG: Self-state configurations are observable using clinical office equipment (fNIRS, EEG) rather than requiring expensive MRI/MEG/PET, enabling real-time monitoring of state transitions.
- Transition Biomarkers: Shifts between self-states produce detectable changes in neural connectivity patterns, particularly in widespread hyperconnectivity patterns characteristic of dissociative subtypes (Yilmaz et al., 2023). Work on neural rigidity in people with autism has shown that different mental states can be computer, and timed, targeted stimulation with TMS—a technique called "brain state-driven neural stimulation" (BDNS)—can increase neural flexibility, as demonstrated by improved performance on task switching, visual switching (e.g. duck-rabbit optical illusion) and social perception (Watanabe, 2025).
Subjective Experience Optimization and Neuroplasticity
The quality of subjective experience during psychotherapy—specifically the optimization of receptive, curious, and non-defensive states—may correlate with measurable neuroplasticity markers. Building on EFT's emphasis on experiential fields, we hypothesize that specific subjective states enhance therapeutic learning through optimized neural plasticity windows. Understanding what experiential states are correlated with increased plasticity, and determining how to identify and induce those states, would be expected to enhance therapeutic efficiency, and potential neuroprotective and regenerative effects for prevention and antiaging (e.g. Guidetti et al., 2022; Caballero-Villarraso et al., 2022; Dufor, Lohof & Sherrard, 2023; Oberman & Benussi, 2024), both requiring further investigation to develop effective, predictable interventions.
Core Hypotheses:
- Experience-Plasticity Correlation: Subjective quality of therapeutic experience correlates with real-time neuroplasticity markers (BDNF, LTP signatures, gamma coherence patterns) to maximize “experience-dependent neuroplasticity” (Kleim & Jones, 2008).
- Plasticity Enhancement: Real-time monitoring of plasticity markers can guide patients toward optimal psychodynamic learning states through biofeedback and various types of neuromodulation, both synchronously and asynchronously. Less intrusive approaches are more amenable for use during therapeutic interventions (e.g. tDCS, tACS), as contrasted with TMS, during which conversation is interrupted by repeating pulse trains. However, for TMS, in-session interventions can be used, including specific meditation practices such as compassion and loving-kindness meditation, mindfulness meditation, and therapeutic approaches such as Exposure and Response Prevention (ERP). Hippocampal-Network TMS (HNT) has been shown in pilot studies to enhance extinction of fear-based memories in PTSD (e.g. Dezachyo et al., 2025).
- Metaplasticity Optimization: Repeated exposure to optimized experiential states enhances long-term capacity for therapeutic change (metaplasticity), measurable through connectivity changes. Understanding the timing, type and sequencing of modulation will be important in developing mature approaches. For instance, transcranial focused ultrasound (tFUS) has been shown to both prime and abolish metaplasticity using theta burst stimulation to primary motor cortex (Ding et al., 2024). Research, reviewed in Popovic and Dragic (2025), has also found that rTMS not only modulates structural plasticity through TrkB-BDNF and MAPK-mTOR pathways, it also has been shown to alter spinogenesis and synaptogenesis, for instance shifting maturation and distribution of different dendritic spine types in key brain areas.
AIT-Based Neural Signatures
Active Inference Therapy's emphasis on Bayesian updating and top-down predictive processing may have identifiable neural correlates, particularly in hierarchical cortical networks. The model's focus on minimizing prediction errors through improved internal modeling presents opportunities for both monitoring and intervention using cortical monitoring (e.g. fNIRS and EEG).
Core Hypotheses:
- Bayes-Optimal Processing Signatures: Effective AIT processing correlates with enhanced top-down connectivity from prefrontal cortex to sensory regions, reflecting improved predictive modeling. Improving top-down error prediction and correction would be expected to improve therapeutic outcomes related to inference-efficiency.
- Error Minimization Patterns: Successful therapeutic updating produces measurable reductions in prediction error signals, particularly in salience network activity.
- Hierarchical Integration: AIT effectiveness correlates with improved integration across temporal hierarchies, from fast sensory updating to ultraslow self-model revision.
- Therapeutic Markov Blanket Function: Successful therapy correlates with achievement of causal sufficiency within the patient-therapist dyad, measurable through enhanced connectivity in causal reasoning networks (DLPFC, posterior parietal cortex) during sessions. Measuring both patient and therapist neural signatures and facilitating optimal synchronisation would be expected to improve dyadic function within the therapeutic system. Wireless EEG, for example, has been used to measure synchrony in musical duets (Zamm et al., 2021), and applications have been discussed for psychotherapy and mental disorders (e.g. Kool et al., 2016; Konrad et al., 2024).
- Causal Model Refinement: Treatment-resistant patients show improved performance on computational causal discovery tasks following AIT, with neural signatures indicating enhanced capacity to distinguish genuine causal relationships from spurious correlations in psychological and interpersonal domains.
Integrated Tripartite Signatures
The convergence of PSSM structural integration, EFT experiential optimization, and AIT mechanistic updating may produce identifiable common neural signatures representing successful therapeutic integration.
Core Hypotheses:
- Common Integration Signature: Successful integration across all three frameworks correlates with specific connectivity patterns reflecting optimal balance between DMN, CEN, and salience networks.
- Temporal Coordination: Integration success correlates with improved temporal coordination across hierarchical time scales (Buzsáki, 2025), reflecting enhanced poly-temporal coherence.
- Plasticity Window Synchronization: Optimal therapeutic moments show synchronized neuroplasticity markers across structural (PSSM), experiential (EFT), and mechanistic (AIT) domains.
Toward "Surgical" Interventional Psychiatry
The ultimate goal involves developing a precision medicine model for psychotherapy and neuromodulation that operates with surgical-level precision in targeting specific neural networks and psychological structures to arrive at a range of desirable end-states.
Building on TAP's network-aligned approach, we propose a comprehensive model where:
- Target State Definition: Clear specification of desired neurobiological and psychological end states for individual patients. End-states may be, for example, functional network configurations, updated complex processes governing psychological function, patient-therapist operating modes, and related measurable outcomes.
- Precision Identification: Individual patient mapping of optimal future states using multimodal assessment;
- Pathway Mapping: Bespoke trajectories from current dysconnectivity to achieving desirable euconnectivity configurations to “update the brain’s operating system”;
- Sequential Intervention Design: Coordinated timing of combined modalities (TMS, psychotherapy, lifestyle interventions) in optimized sequence with continuous performance improvement (CPI);
- AI Digital Twinning: Virtual patient, therapist and dyadic modeling to simulate and optimize treatment pathways;
- Real-Time Monitoring: Continuous assessment and trajectory adjustment during and between interventions;
- Agentic AI Coaching: Automated patient support with minimal human oversight;
- Multimodal Coaching Applications: Sophisticated behavioral-to-psychodynamic AI interfaces;
- Integrated Care Coordination: AI systems providing feedback to optimize human clinician collaboration.
These hypotheses require systematic empirical validation through carefully designed studies that can capture the complexity of integrated neuromodulation-psychotherapy approaches while maintaining methodological rigor. Given the wide range of possibilities in a newly evolving field combined with massive unmet mental health needs in the population, and functionally infinite research avenues require careful consideration. Review, selection and design, given limited resources, ought to focus on approaches which are most clinically-accessible and likely to result in greatest benefit. Therefore, office-based technologies which are easier to learn and implement should take precedence over complex and costly systems which are unlikely to translate to clinical practice. Additional measures, such as heart rate variability and related physiological measures, have not been discussed in detail but may play an important role in sophisticated assessment and treatment protocols.
Limitations and Future Work
Limitations include empirical gaps: synergies speculate without direct testing (e.g., neural correlates of "entanglement" via generalised synchrony), risking over-reliance on metaphors requiring more precise formalism, and incorporation of precise neuronal dynamics in hierarchical top-down and bottom-up interactions as elaborated by others with greater knowledge and technical ability. Future work could test hypotheses like AIT's inference and learning — i.e., changes in induced responses and effective connectivity — in fMRI, EEG or fNIRS, or PSSM's scales correlating with lifespan topology via RCTs in a more typical clinical trial model, requiring elaboration of a practical framework for application and testing.
Neuronal-Level Dynamics: A Brief Note on Potential Elaboration
While the tripartite model emphasizes network-level processes—such as hierarchical connectivity patterns in fronto-limbic circuits, temporal synchronization across scales (Buzsáki, 2025), and entropy-mediated plasticity (Carhart-Harris & Friston, 2019)—a deeper integration of neuronal-level details could further enrich its explanatory power. At this granular scale, mechanisms like spike-timing-dependent plasticity (STDP) in pyramidal neurons, dopaminergic modulation of synaptic weights in cortical-striatal loops, or GABAergic inhibition regulating prediction error signals (as in AIT's Bayesian updating) might underpin the model's core synergies. For instance, dissociated self-states in PSSM could arise from impaired dendritic integration or silent synapses in prefrontal and hippocampal neurons, resolved through LTP induction during EFT's co-created fields. Similarly, Freud's "psychical entropy" (1937) might manifest neuronally as reduced variability in firing patterns, with therapy promoting burst firing to enhance adaptive reorganization.
However, such neuronal elaboration is beyond the scope of this paper, which prioritizes a meta-framework accessible to clinical practice and empirical testing at the network level. Current monitoring technologies—such as EEG for oscillatory coherence, fNIRS for hemodynamic responses, or TMS/tDCS for neuromodulation—provide indirect proxies of brain activity but do not directly access single-neuron dynamics or neurotransmitter systems (e.g., real-time dopamine or serotonin fluctuations). These tools excel at capturing large-scale network signatures, like gamma-band synchrony for relational entanglement or dysconnectivity in dissociative states (Lanius et al., 2018), (Edwards et al., 2012; Parees et al., 2014) but lack the resolution for cellular or molecular insights without invasive methods (e.g., single-unit recordings or PET imaging of neurotransmitters), which are impractical in routine clinical settings.
Future work could bridge this gap through computational modeling (e.g., simulating neuronal ensembles via tools like NEURON or the Virtual Brain) or advanced techniques like optogenetics in preclinical studies, potentially informing "surgical" interventions. Nonetheless, the model's strength lies in its network-level applicability, leaving neuronal precision as a promising avenue for specialized collaborators to explore in subsequent refinements. The neuromodulation-integration hypotheses require validation through studies that can demonstrate causal relationships between targeted neural interventions and psychological outcomes, moving beyond correlational findings to establish mechanistic understanding of how combined approaches enhance therapeutic efficacy.
References
Bass, A. (2001). Difference and disavowal: The trauma of Eros. Stanford University Press.
Bion, W. R. (1962). Learning from experience. Heinemann.
Borg, M., Jr., Brenner, G. H., & Berry, D. (2022). Making your crazy work for you: From trauma to self-healing. Central Recovery Press.
Brenner, G. H. (2010). To speak or not to speak—The taboo of communication. Journal of Gay & Lesbian Mental Health, 14(3), 230–239.
Brenner, G. H. (2025). Active Inference Therapy: A first-principles framework for psychotherapeutic intervention. Neuromodec Journal.
Brenner, G. H., Ufearo, S., & Zhou, M. (2025). Transcranial magnetic stimulation–assisted psychotherapy (TAP): Toward a paradigm shift. Neuromodec Journal.
Bridgman, Percy Williams, 1927. The Logic of Modern Physics, New York: Macmillan.
Bromberg, P. M. (1995). Standing in the spaces: The multiplicity of self and the psychoanalytic relationship. Contemporary Psychoanalysis, 31(4), 509–535.
Bromberg, P. M. (1998). Standing in the spaces: Essays on clinical process, trauma, and dissociation. Analytic Press.
Buzsáki, G. (2025). Rhythms of the brain (2nd ed.). Oxford University Press.
Caballero-Villarraso J, Medina FJ, Escribano BM, Agüera E, Santamaría A, Pascual-Leone A, Túnez I. Mechanisms Involved in Neuroprotective Effects of Transcranial Magnetic Stimulation. CNS Neurol Disord Drug Targets. 2022;21(7):557-573. doi: 10.2174/1871527320666210809121922. PMID: 34370648.
Carhart-Harris, R. L., Leech, R., Hellyer, P. J., Shanahan, M., Feilding, A., Tagliazucchi, E., Chialvo, D. R., & Nutt, D. (2014). The entropic brain: A theory of conscious states informed by neuroimaging research with psychedelic drugs. Frontiers in Human Neuroscience, 8, 20.
Carhart-Harris, R. L., & Friston, K. J. (2019). REBUS and the anarchic brain: Toward a unified model of the brain action of psychedelics. Pharmacological Reviews, 71(3), 316–344.
Chamberlin, D. E. (2023). The Active Inference Model of Coherence Therapy. Frontiers in Human Neuroscience, 16, 955558.
Dezachyo, O., Yair, N., Mendelovich, N., Tik, N., Pine, D. S., Sharon, H., Tavor, I., Bar-Haim, Y., & Censor, N. (2025). Hippocampal-network transcranial magnetic stimulation to target reactivated intrusive memories: A proof-of-concept study in PTSD treatment. Brain Stimulation: Basic, Translational, and Clinical Research in Neuromodulation, 18(6), 1993-1995. https://doi.org/10.1016/j.brs.2025.10.019
Ding MYR, Arora T, Sarica C, Yang AZ, Nasrkhani N, Grippe T, Nankoo JF, Tran S, Samuel N, Xia X, Lozano AM, Chen R. Investigation of Metaplasticity Associated with Transcranial Focused Ultrasound Neuromodulation in Humans. J Neurosci. 2024 Oct 30;44(44):e2438232024. doi: 10.1523/JNEUROSCI.2438-23.2024. PMID: 39266303; PMCID: PMC11529810.
DID-Research.org. (2024, June 21). Structural dissociation. Retrieved December 23, 2025. https://did-research.org/origin/structural_dissociation/
Dufor, T., Lohof, A. M., & Sherrard, R. M. (2023). Magnetic Stimulation as a Therapeutic Approach for Brain Modulation and Repair: Underlying Molecular and Cellular Mechanisms. International Journal of Molecular Sciences, 24(22), 16456. https://doi.org/10.3390/ijms242216456
Edwards, M.J., Adams, R.A., Brown, H., Parees, I., Friston, K.J., 2012. A Bayesian account of 'hysteria'. Brain 135, 3495-3512.
Freud, S. (1912). Recommendations to Physicians Practising Psycho-Analysis. In J. Strachey (Ed. & Trans.), The Standard Edition of the Complete Psychological Works of Sigmund Freud (Vol. 12, pp. 109–120). London: Hogarth Press.
Freud, S. (1937). Analysis terminable and interminable. In J. Strachey (Ed. & Trans.), The standard edition of the complete psychological works of Sigmund Freud (Vol. 23, pp. 209–253). Hogarth Press.
Freud, S. (1950 [1895]). Project for a Scientific Psychology. In J. Strachey (Ed.), The Standard Edition of the Complete Psychological Works of Sigmund Freud (Vol. 1, pp. 281–391). London: Hogarth Press.
Friston, K. (2010). The free-energy principle: A unified brain theory? Nature Reviews Neuroscience, 11(2), 127–138.
Friston, K. J., & Frith, C. D. (2015). A Duet for One: Predictive Coding and Active Inference in the Brain. Consciousness and Cognition, 36, 390–405.
Friston, K. J., Stephan, K. E., Montague, R., & Dolan, R. J. (2014). Computational psychiatry: The brain as a phantastic organ. The Lancet Psychiatry, 1(2), 148–158.
Friston, K.J., Frith, C.D., 2015. Active inference, communication and hermeneutics. Cortex; a journal devoted to the study of the nervous system and behavior 68, 129-143.
Friston, K., Parr, T., & de Vries, B. (2022). Active inference. MIT Press.
Gadamer, H.-G. (1975). Truth and Method (2nd ed., Trans. J. Weinsheimer & D. G. Marshall). New York: Continuum.
Guidetti M, Bertini A, Pirone F, Sala G, Signorelli P, Ferrarese C, Priori A, Bocci T. Neuroprotection and Non-Invasive Brain Stimulation: Facts or Fiction? Int J Mol Sci. 2022 Nov 9;23(22):13775. doi: 10.3390/ijms232213775. PMID: 36430251; PMCID: PMC9692544.
Griffiths TA, Dimitrova LI, Linington M, Terhune DB, Reinders AATS. Effectiveness of phase-oriented treatment for trauma-related dissociative disorders: a systematic review. Eur J Psychotraumatol. 2025 Dec;16(1):2545734.
He, H., Sun, X., Doose, J., Faller, J., McIntosh, J. R., Saber, G. T., Huffman, S., Hong, L., Pantazatos, S. P., Yuan, H., McTeague, L. M., Goldman, R. I., Brown, T. R., George, M. S., & Sajda, P. (2025). TMS-induced modulation of brain networks and its associations to rTMS treatment for depression: A concurrent fMRI-EEG-TMS study. Brain Stimulation: Basic, Translational, and Clinical Research in Neuromodulation, 18(6), 1955–1965.
Hohwy, J., 2016. The Self-Evidencing Brain. Nous 50, 259-285.
Holmes, J., & Nolte, T. (2019). "Surprise" and the Bayesian brain: Implications for psychotherapy theory and practice. Frontiers in Psychology, 10, 592. https://doi.org/10.3389/fpsyg.2019.00592
Holmes J. Friston, Free Energy, and Psychoanalytic Psychotherapy. Entropy (Basel). 2024 Apr 18;26(4):343. doi: 10.3390/e26040343. PMID: 38667897; PMCID: PMC11049609.
Kita, A., Ishida, T., Kita, N., et al. (2025). Exploring the capabilities of repetitive transcranial magnetic stimulation in major depressive disorder: Dynamic causal modeling of the neural network. Translational Psychiatry, 15, 257.
Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res. 2008 Feb;51(1):S225-39. doi: 10.1044/1092-4388(2008/018). PMID: 18230848.
Kluft, R. P., & Fine, C. G. (Eds.). (1993). Clinical perspectives on multiple personality disorder. American Psychiatric Press.
Konrad K, Gerloff C, Kohl SH, Mehler DMA, Mehlem L, Volbert EL, Komorek M, Henn AT, Boecker M, Weiss E, Reindl V. Interpersonal neural synchrony and mental disorders: unlocking potential pathways for clinical interventions. Front Neurosci. 2024 Mar 11;18:1286130. doi: 10.3389/fnins.2024.1286130. PMID: 38529267; PMCID: PMC10962391.
Koole, S. L., & Tschacher, W. (2016). Synchrony in psychotherapy: A review and an integrative framework for the therapeutic alliance. Frontiers in Psychology, 7, Article 862.
Lagasse, E., & Levin, M. (2023). Future medicine: From molecular pathways to the collective intelligence of the body. Trends in Molecular Medicine, 29(9), 687-710.
Lanius, R. A., Boyd, J. E., McKinnon, M. C., Nicholson, A. A., Frewen, P., Vermetten, E., Jetly, R., & Spiegel, D. (2018). A review of the neurobiological basis of trauma-related dissociation and its relation to cannabinoid- and opioid-mediated stress response: A transdiagnostic, translational approach. Acta Psychiatrica Scandinavica, 138(6), 489-517.
Leichsenring, F., Abbass, A., Heim, N., Keefe, J.R., Kisely, S., Luyten, P., Rabung, S. and Steinert, C. (2023), The status of psychodynamic psychotherapy as an empirically supported treatment for common mental disorders – an umbrella review based on updated criteria. World Psychiatry, 22: 286-304.
Levin, M. (2019). The Computational Boundary of a “Self”: Developmental Bioelectricity and the Origin of Primitive Cognition. Frontiers in Psychology, 10, 2688.
Levin, M. (2021). Bioelectrical approaches to cancer as a problem of the scaling of the cellular self. Progress in Biophysics and Molecular Biology, 165, 102–113.
Maturana, H. R., & Varela, F. J. (1980). Autopoiesis and cognition: The realization of the living (R. S. Cohen & M. W. Wartofsky, Eds.; 2nd ed.). Springer.
Mousley, A., Bethlehem, R.A.I., Yeh, FC. et al. Topological turning points across the human lifespan. Nat Commun 16, 10055 (2025). https://doi.org/10.1038/s41467-025-65974-8
Oberman LM, Benussi A. Transcranial Magnetic Stimulation Across the Lifespan: Impact of Developmental and Degenerative Processes. Biol Psychiatry. 2024 Mar 15;95(6):581-591. doi: 10.1016/j.biopsych.2023.07.012. Epub 2023 Jul 29. PMID: 37517703; PMCID: PMC10823041.
Ogden, T. H. (1994). The analytic third: Working with intersubjective clinical facts. International Journal of Psychoanalysis, 75, 3-19.
Parees, I., Brown, H., Nuruki, A., Adams, R.A., Davare, M., Bhatia, K.P., Friston, K., Edwards, M.J., 2014. Loss of sensory attenuation in patients with functional (psychogenic) movement disorders. Brain 137, 2916-2921.
Petersen, E., & Ursin, F. (2025). Against disease classification: Toward continuous disease assessment in precision medicine. NEJM AI, 3(1), AIp2500873.
Popovic, D., & Dragic, M. (2025). Repetitive transcranial magnetic stimulation as a universal modulator of synaptic plasticity: Bridging the gap between functional and structural plasticity. Neurochemistry International, 188, 106021.
Reinders, A. A. T. S., Chalavi, S., Schlumpf, Y. R., Vissia, E. M., Nijenhuis, E. R. S., Jäncke, L., Veltman, D. J., & Stein, D. J. (2018). Aiding the diagnosis of dissociative identity disorder: Pattern recognition study of brain biomarkers. The British Journal of Psychiatry, 213(3), 541-547.
Ross, R. M., Heilicher, M., Palombo, D. J., McKinnon, M. C., & Lanius, R. A. (2021). The dissociative subtype of posttraumatic stress disorder is associated with subcortical white matter network alterations. Brain Imaging and Behavior, 15(3), 1402-1410.
Saxe, G. N., Bickman, L., Ma, S., & Aliferis, C. (2022). Mental health progress requires causal diagnostic nosology and scalable causal discovery. Frontiers in Psychiatry, 13, 898789.
Saxe, G. N., Ma, S., Morales, L. J., Galatzer-Levy, I. R., Aliferis, C., & Marmar, C. R. (2020). Computational causal discovery for post-traumatic stress in police officers. Translational Psychiatry, 10(1), 233.
Schwartz, R. C. (1995). Internal family systems therapy. Guilford Press.
Seligman, S. (2005). Dynamic Systems Theories as a Metaframework for Psychoanalysis. Psychoanalytic Dialogues, 15(2), 285–319.
Shedler J. The efficacy of psychodynamic psychotherapy. Am Psychol. 2010 Feb-Mar;65(2):98-109. doi: 10.1037/a0018378. PMID: 20141265.
Shen, Y.L., Hyon, R., Wheatley, T. et al. Neural similarity predicts whether strangers become friends. Nat Hum Behav 9, 2285–2298 (2025). https://doi.org/10.1038/s41562-025-02266-7
Solms, M. (2018). The scientific standing of psychoanalysis. BJPsych International, 15(1), 5–8.
Solms, M., & Nersessian, E. (1999). Freud's theory of affect: Questions for neuroscience. Neuro-Psychoanalysis, 1(1), 5-14.
Solms, M., & Panksepp, J. (2012). The “Id” Knows More than the “Ego” Admits: Neuropsychoanalytic and Primal Consciousness Perspectives on the Interface between Affective and Cognitive Neuroscience. Brain Sciences, 2(2), 147–175.
Solms, M. (2020). New project for a scientific psychology: General scheme. Neuropsychoanalysis, 22(1–2), 5–35.
Solms, M. (2024) The mechanism of change in the ‘talking cure’: A neuropsychoanalytic perspective. In S. Gullestad, E. Stänicke, M. Leuzinger-Bohleber (eds.), Psychoanalytic Studies of Change: An Integrative Perspective, London: Routledge, pp. 114-127.
Solms, M. (2026). The only cure: Freud and the neuroscience of mental healing. Avid Reader Press / Pegasus.
Steele, K., van der Hart, O., & Nijenhuis, E. R. S. (2005). Phase-oriented treatment of structural dissociation in complex traumatization: Overcoming trauma-related phobias. Journal of Trauma & Dissociation, 6(3), 11-53.
Stern, D. N. (2009). The present moment in psychotherapy and everyday life. Norton.
Tschacher, W., Giersch, A., Friston, K., 2017. Embodiment and Schizophrenia: A Review of Implications and Applications. Schizophr Bull 43, 745-753.
Tschacher, W., Haken, H., 2007. Intentionality in non-equilibrium systems? The functional aspects of self-organized pattern formation. New Ideas in Psychology 25, 1-15.
van der Hart, O., Nijenhuis, E. R. S., & Steele, K. (2006). The Haunted Self: Structural Dissociation and the Treatment of Chronic Traumatization. New York: W. W. Norton.
Watanabe, T., Yamasue, H. Noninvasive reduction of neural rigidity alters autistic behaviors in humans. Nat Neurosci 28, 1348–1360 (2025). https://doi.org/10.1038/s41593-025-01961-y
Winnicott, D. W. (1953). Transitional Objects and Transitional Phenomena. International Journal of Psycho-Analysis, 34, 89–97.
Yilmaz, T., Ravi, M., Palaniyappan, L., Kish, S. J., Kundu, P., Meyer, J. H., Houle, S., Husain, M. I., & Blumberger, D. M. (2023). Large-scale functional hyperconnectivity patterns in trauma-related dissociation: An rs-fMRI study of PTSD and its dissociative subtype. Nature Mental Health, 1(10), 690-703.
Zamm A, Palmer C, Bauer AR, Bleichner MG, Demos AP, Debener S. Behavioral and Neural Dynamics of Interpersonal Synchrony Between Performing Musicians: A Wireless EEG Hyperscanning Study. Front Hum Neurosci. 2021 Sep 13;15:717810. doi: 10.3389/fnhum.2021.717810. PMID: 34588966; PMCID: PMC8473838.
Read this next
What Silicon Valley needs to know about the brain, and what it doesn't - Part I
Silicon Valley wants to get inside your head - literally. While these projects adopt mixes of commercial stealth and elaborate publicity, and the breadth of applications spans the entire human condition, all these technologies take one of two product forms: Either as a chip implanted in your head transmitting to a computer or as a wearable cap transmitting to a computer.
Neuromodulation for COVID-19, Neuromodec update 10: Major steps forward
This is the 10th update from Neuromodec (August 7, 2023) on the use of Neuromodulation for COVID-19 as part of Neuromodec’s initiative to educate on and advance treatments.
Perspective by Dr. Kip Ludwig: What does the recent Neuralink FDA IDE really mean?
No matter what, getting an Investigational Device Designation (IDE) for a brain implant from the Food and Drug Administration (FDA) isn’t trivial...
